AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2768-0487/035
*Corresponding Author: Rosita Fontes, Endocrinology Service, Diagnosticos da America SA (DASA), Thyroid Department, Instituto Estadual de Diabetes e Endocrinologia Luiz Capriglione (IEDE).
Citation: : R Fontes, M M Negri, S Marui, Y Schrank, AFDF Perozo, et al. (2021) A higher cut-off for Thyroid-stimulating immunoglobulin (TSI) could better predict relapse in Graves’ disease?. Journal of Clinical and Laboratory Research. 3(2); DOI:10.31579/2768-0487/035
Copyright: ©2021 Rosita Fontes. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 July 2021 | Accepted: 05 August 2021 | Published: 09 August 2021
Keywords: TSI; hyperthyroidism; diagnosis; treatment
Background: TSH receptor (TSHr)-stimulating immunoglobulins (Igs) can be used as diagnostic markers of Graves’ disease (GD). Thyroid-stimulating immunoglobulin (TSI) assays exclusively detect these specific Igs. Materials and Methods: This was a prospective longitudinal study in which hyperthyroid patients with GD and toxic nodular goitres were evaluated at diagnosis. GD patients were also evaluated at antithyroid drug (ATD) withdrawal. An automated chemiluminescent assay measured TSI. According to the manufacturer TSI less than 0.55 IU/L was a non-reactive result. The authors evaluated the Se and Sp of the cutoff point provided by the TSI assay manufacturer, and tested other cutting points through a ROC curve, to assess relapse risk of Graves’ disease. Results: At diagnosis, were evaluated 92 (85.2%) GD patients aged 41.2 ± 2.0 years, and 16 patients (14.8%) with toxic multinodular goiter (TMNG) or toxic adenoma (TA), aged 60.8 ± 4.8 years. They were re-evaluated after 18 ± 4 months with methimazole (MMI) treatment. The follow-up after treatment suspension was of 20 ± 6 months. At diagnosis, the TSI (Se) and (Sp) were 98.9% and 100%, respectively. At ATD withdrawal, despite a high Se (95.5%), Sp was low (59.6%). By adjusting the cut-off to 1.11 (TSI <1.11 IU/L non-reactive), TSI presented the best Sp (89.4%) with a small decrease in Se (93.3%) in predicting GD relapse. Conclusions: TSI had high Se and Sp in GD differential diagnosis with nodular goiters. In the assessment for GD relapse, by raising the cutting point to 1.11 IU/L, a better Sp was obtained at the expense of a small drop in Se. A larger sample is needed to support a higher TSI cut-off point in the clinical routine to assess GD relapse after ATD.
Hyperthyroidism is a consequence of excessive thyroid hormone production by the thyroid gland. In iodine sufficient areas, the most common cause of hyperthyroidism is Graves’ disease (GD), responsible for about 80% of cases [1, 2]. GD is an autoimmune disease mediated by immunoglobulins (Igs) that activate the TSH receptor (TSHr). This leads to TSH-independent thyroid hyperplasia and unregulated thyroid hormone (TH) production and secretion, usually accompanied by goiter [3]. It follows in frequency as causes of hyperthyroidism, toxic multinodular goiter (TMNG) and toxic adenoma (TA), that become autonomous producing TH independent of stimulus from either TSH or TSHr antibodies [4, 5].
As GD is an autoimmune disease, patients can experience relapse after stopping anti-thyroid drugs (ATD) [6]. The relapse rate after ATD withdrawal can reach 50%, depending on several factors. Measurement of TSHr stimulatory Igs can be an indirect indicator of GD activity, and be useful when assessing the prognosis [1, 7].
The thyrotropin receptor antibody (TRAb) assays measure both thyroid-stimulating and thyroid-blocking Igs. These assays have been more used in special situations in which there is doubt about GD diagnosis. At the end of treatment, for relapse prediction, there could be doubt about ATD withdrawal when using this test, because TRAb can also detect TSHr-blocking Igs [8, 9].
The thyroid-stimulating immunoglobulin (TSI) assays measure only stimulating Igs. Thyrotoxicosis by GD is caused by stimulus of TSHr by these Igs, theoretically TSI assays would be the best marker of the disease, and should be capable of better predicting relapse [10, 11].
Laboratory and retrospective clinical studies of TSI performance compared with TRAb showed a good correlation between the two tests [6, 11, 12, 13, 14, 15]. However, there are still too few prospective studies following GD patients to judge whether the TSI performance can accurately predict hyperthyroidism relapse after ATD treatment in GD.
This study aimed to evaluate, prospectively, autoimmunity before treatment for GD, TMNG and TA, and recurrence risk and at the end of treatment with ATD for GD, through TSI measurement.
This is a prospective longitudinal study performed in a tertiary care service specialized in treating thyroid diseases of a sufficient iodine region [16, 17]. The inclusion criteria [1,2] were: age 20 years and over, suppressed TSH, and free T4 (FT4) and total T3 (TT3) above the reference intervals (RI), with symptoms and signs of hyperthyroidism for more than 3 months, presence of goiter, with or without GD ophthalmopathy, of any gender. An ultrasound examination of the thyroid determined if goiter was diffuse or nodular. Those with nodular goiter underwent thyroid scintigraphy: if there was an increase in 131I uptake in the corresponding region to one or more nodules, they were included as TA or TMNG [4]. Before being included in the study, hormonal measurements were confirmed in more than one blood sample.
Exclusion criteria were age below 20 years, GD ophthalmopathy candidates for treatment with glucocorticoids, need for hospitalization due to the hyperthyroidism severity, pregnancy, postpartum period of up to 6 months, and use of medicines known as possible analytical or physiological interference on the measurement of TSH and/or TH in the past 3 months (medicines and contrasts containing iodine and amiodarone in the past 6 months) [6, 8].
TSH and TH were measured in patients with untreated GD, TMNG or TA before starting treatment with ATD. Once starting treatment, these hormones were measured after 1, 2, and 3 months, and every 4 months, or at shorter intervals as needed [2]. GD patients were followed until they reached criteria for discontinue ATD; BMNT and TA were followed until the definitive treatment. During treatment, the patients were seen at the thyroid specialized clinical, and everyone maintained contact with the main researcher to communicate any adverse effects or other factors that could lead to treatment interruption or non-adherence.
GD patients were evaluated again at the time of ATD withdrawal if they meet all the following criteria: 1) at least 12 to 24 months of treatment; 2) clinical euthyroidism in the last 3 months, and in use of low ATD dose during this period; 3) TSH not suppressed and within the reference interval (RI); and 4) normal FT4 and TT3 [2].
After withdrawing the medication, hormonal measurements were repeated after 1, 2, and 4, and then every 4 months until at least 24 months if patients did not relapse [2]. If during the follow-up period they presented symptoms and signs compatible with hyperthyroidism they were considered for relapse and were reassessed at any time other than planning. If they had a relapse, the TSI and hormonal measurements were repeated at the time of relapse diagnosis. GD relapse was considered if it occurred within at least 12 months after ATD discontinuation. Until February 2020, patients were followed up at the thyroid clinic to confirm clinical euthyroidism and perform the tests. Between March 2020 and March 2021 they were evaluated by teleconsultations due to the COVID-19 pandemic. From March to June 2021 they were again followed at the thyroid clinic. Hormonal and TSI measurements were interrupted between March and July 2020 when the laboratory unit responsible for blood collection was closed for public assistance. During this period, some revaluations were delayed by about 4 months.
TSI was determined by a chemiluminescent assay (Immulite 2000, Siemens Healthcare Diagnostics Inc), with a mean intra-assay percentage coefficient of variation (% CV) of 6.0%. According to the manufacturer, TSI less than 0.55 IU/L was a non-reactive result. TRAb was measured by an electrochemiluminescent assay in Modular Analytics® E170, Roche Diagnostics Ltd, with amean intra-assay % CV of 5.7%. According to the manufacturer, TRAb less than 1.75 IU/L was a non-reactive result. Serum TSH (immunometric assay), FT4, and TT3 (competitive assays) were measured by electrochemiluminescence by Roche Diagnostics Ltd. The TSH interval reference (RI) was 0.4–4.3 mIU/L (20 to 59 years), 0.4–5.8 mIU/L (60 to 79 years), and 0.4–6.7 mIU/L (80 years and over). TSH was suppressed if < 0>
R software (version 4.0.1) was used to perform all statistical calculations [19, 20]. We tested the sensitivity (Se) and specificity (Sp) of the TSI assay for the differential diagnosis between DG and TMNA/TA, and for prediction of relapse at the end of GD treatment using the cut-off point provided by the manufacturer. We tested other cut-off points that could provide a better Sp without Se prejudice, using a ROC curve. To assess the normal distribution of the data, Kolmogorov-Smirnov tests were performed. Data were log-transformed (base 10) before analysis for analytes with non-normal distribution. Means and standard deviations were used to demonstrate continuous variables. A two-tailed Mann-Whitney test was used to compare the nonparametric TSI and TSH distributions. The student’s t-test was used in the case of two data series with a normal distribution. The levels of analytes below the limit of quantification were considered one-hundredth below the limit of quantification for statistical analysis. The level of significance used was 0.05.
The study was approved by the Research Ethics Committee of the Instituto Estadual de Diabetes e Endocrinologia Luiz Capriglione (IEDE), CAAE 90325418.5.0000.5266. The invited subjects agreed to participate by signing the informed consent form.
Of 124 patients, five were excluded before onset due to severe GD ophthalmopathy who needed glucocorticoid treatment. Of the remaining 119 who started the study, 11 did not complete: four because of non-adherence to treatment; two because they moved to another city; one became pregnant; and four due to the difficulty in controlling hyperthyroidism with ATD (of these, three were submitted to 131I treatment, and one has undergone surgery). One patient was a male transgender and was not excluded from the study.
Of the 108 patients selected, 92 (85.2%) had GD, and 16 had TMNG or TA (14.8%). Age and gender by groups are in table 1. All patients were treated with methimazole (MMI). The initial MMI dose for GD ranged from 20 to 40 mg/day, and they had a titration according to clinical and laboratory evaluation during periodic visits. They were treated for 18 ± 4 months (14-26) until clinical and laboratory parameters were reached. The MMI dose used at the time of treatment discontinuation was 2.5 – 5.0 mg/day. Those with TMNG or TA were treated with 10 -20 mg/day until the definitive treatment was done.
After ATD withdrawal GD patients had a follow-up 20 ± 6 months (12–30). Laboratory data before treatment are in Table 1. Data of the TSI performance for predicting relapse after treatment with ATD are in Table 2. In those who presented relapse, it occurred in 4 ± 3 months (2-11) after ATD withdrawal. At that time there was no statistically significant difference in age, TSH, FT4, or TT3 levels between groups that relapsed or not (p = 0. 469581, p = 0.432298, p = 0.467808, p = 0.769889, respectively).
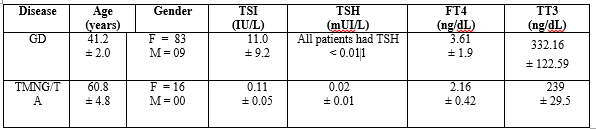
Legend: GD: Graves` disease; TMNG: toxic multinodular goiter; TA: toxic adenoma; ATD: anti-thyroid drug; TSI: Thyroid stimulating immunoglobulin; TSH: Thyroid-stimulating hormone; FT4: free T4; TT3: Total T3.
The results are presented as means and standard deviations

N: Number of cases; TSI: Thyroid stimulating immunoglobulin; TSH: Thyroid Stimulating hormone; FT4: free T4; TT3: Total T3.
The results are presented as means and standard deviations
At the time of ATD withdrawal of GD patients, TSI levels were significantly higher in patients who experienced relapse than in those who had no relapse (p = 0.0135). The TSI Se and Sp to predict relapse are in Table 3. Since TRAb was the test routinely used at that time to assess autoimmunity, the results are also shown for comparison to TSI. Assessing possible other cut-off points for the TSI that could better predict the GD recurrence, a ROC curve (image not included) demonstrated that an adjustment of the cutoff to 1.1 IU/L (TSI < 1>
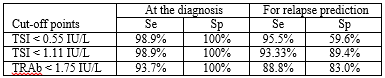
TSI: Thyroid stimulating immunoglobulin; TRAb: thyrotropin receptor antibody; Se: Sensitivity; Sp: Specificity
The average remission rate after a course of ATD for GD is about 50% [21]. Some factors may be associated with a higher relapse rate. One factor is the high concentration of Igs capable of stimulating the TSHr. The remission rate is lower if TSHr is elevated before the ATD suspension. [22]. As there are still few studies evaluating GD recurrence with TSI assay [2, 6], we aimed to evaluate the performance of this test in GD patients treated with ATD.
TSHr-stimulating Igs are used as diagnostic markers of GD. The TSI assay only detect Igs capable of stimulating TSHr [2]. Until some years ago, TSI was assessed by bioassays, making it difficult to incorporate the complex and expensive technique into the laboratory routine [23]. In recent years, an automated assay that directly measures TSI has been used, showing high clinical value in preliminary studies [10, 11].
In the present study, we compared results of TSI in patients with GD with those with TMNG or TA at diagnosis, since the latter are not autoimmune diseases. In almost all GD patients TSI was reactive using the cut-off provided by the manufacturer. As expected, all patients with TMNG and TA had TSI non-reactive. In this way, TSI showed high diagnostic Se and Sp for GD diagnosis, of 98.9% and 100%, respectively. These data agree with previous data that show high TSI Se and Sp for GD diagnosis [1, 6, 11, 24].
At the end of treatment, TSI Se and Sp were reassessed to predict GD relapse.
At this stage, a positive result could indicate that autoimmune activity was still present and, therefore, the high probability of disease recurrence due to the presence of Igs capable of stimulating TSHr [25]. The TSI level was higher in patients who relapsed in the following months. Other studies have found similar results, but they were retrospective [6, 26], or performed with the TRAb measurement, an assay which is not specific for the evaluation of TSTr-stimulating Igs [25, 27]. It is also known that patients with higher TRAb-reagent titers are likely to return to hyperthyroidism and should be given the choice of continuation of MMI treatment [8]. It can be inferred that the same happens with the TSI, and that is why it is important to define exactly what level of TSI would indicate that the treatment should be maintained longer.
We observed that some patients who did not relapse had reactive TSI, but near the 0.55 cutoff. This was responsible for the low Sp when assessing ATD withdrawal, despite the high Se. This encouraged the authors to analyze if another cut-off point could lead to a higher Sp without prejudice to the Se. Among the various points tested, the one that showed the best Sp was 1.11 IU/L, at the expense of a very small loss of Se. With this cut-off point, TSI Sp was higher to that of TRAb, still with a similar Se.
In recent years, laboratories are replacing assays that measure TRAb by those that measure TSI in commercial platforms. This is likely because the latter, in addition to being automated, is faster, promoting better cost-benefit to the laboratory routine. At least one study showed that the inclusion of TSI measurement in the current diagnostic algorithms confers cost savings and shortens time to diagnosis [10].
According to the present study, TSI proved to be clinically relevant in the assessment of diagnosis, and in prediction of GD relapse. The data obtained suggest that a higher cut-off point would better contribute to the evaluation for ATD discontinuation. As the still limited number of patients studied can lead to bias, this data now requires validation through other prospective studies.
In this group, TSI had high Se and Sp in the diagnosis of GD and for differential diagnosis with nodular goiters. In the assessment to GD relapse upon suspension of ATD, despite the good Se, a low Sp was obtained with the cut-off provided by the manufacturer. By raising the cutting point to 1.11 IU/L, a higher Sp was obtained at the expense of a small drop in Se, which still remained high. A larger sample is needed to support a higher TSI cut-off point in the clinical routine for the assessment of GD relapse after ATD.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
